


Varian vs. The World: Can Anyone Break Through?: Part 1
A deep dive into the potential of United Imaging's uRT-linac 506c and its challenge to Varian’s reign.

The majority of my career, I have been using Varian’s TrueBeam to treat patients. It is a remarkable machine. It is an absolute workhorse for your typical VMAT/IGRT cases. It can do radiosurgery very well. It has the ability to utilize electrons and obviously can do 3D plans. It has a high dose rate. The imaging with CBCT is great for almost every part of the body, except for the abdomen where the gas patterns make it challenging - this is why I don’t think it is particularly good for hepatobiliary and pancreas tumors, though you can do a decent job with liver SBRT. I absolutely love this machine and other than high dose pancreas and cases suitable for protons, I do everything on it. I also love the contouring on Eclipse (my apologies to MIM users - I just don’t care for the tools, but I do love the fusion) and I like reviewing plans on Eclipse. We don’t use ARIA to its fullest potential, but I find it relatively easy to use - much easier than MOSAIQ (however, I’ve not used the newest version). There is remarkably little downtime and I’ve noted this over the course of >10 years on at least 5 different TrueBeams. The hardware tech support is excellent - what a great team they have. Overall, I stan for Varian products.
There are competing products that I’ve have used that are … fine. They are okay and the work just fine. They get the job done, but in my very subjective opinion, if I have a choice, I would always pick a TrueBeam. Now, if I was considering changing jobs and the practice did not have them, it is not at all a game changer. I would happily take another job if it seemed a better fit even if they did not use Varian products. I would spend the first few months complaining that we didn’t have it and then I would move on with my life.
Now, are their downsides? Yes. They are expensive compared to the other machines. Yes, I think they are better and there is a “value add” for the price differential. However, not every facility has the resources to afford the hardware, software and service contracts and so they may choose another platform to reduce overhead and be able to keep the lights on. That is fine, I completely understand. I don’t find their software support to be very good. The documentation in ARIA is not easily customizable and the summary tables for end of treatments are horrible. As an example, if you treat a few separate brain mets, for whatever reason, it sums the doses even though they are different locations in the brain. I saw a medonc’s note the other day and it said I treated brain mets to a dose of 57 Gy in 8 Fx. I know I may do some of out of the box fractionation, occasionally, but this is simply incorrect. It was a sum of 30 Gy in 5 Fx and 27 Gy in 3 Fx to two separate areas. I don’t love how the weekly management notes look, even after I’ve tried my best to customize, so I do them in EPIC. There is no internal scorecard for dosimetry, so you are forced to buy software like ClearCheck from Radformation and this is annoying. The connection to Microsoft Word can be faulty at times and it creates a lot of issues for me that lead me to reboot. Anyway, all of these cons are mitigated by the fact that it really does great treatments.
Basically, they are a monopoly, or as close to one as can be in our specialty. There are a few other players, but most centers, if well resourced, will purchase TrueBeams. This allows them to keep prices high for hardware, software and service. There really is not an alternative if you want a premium product linear accelerator.
But, there are a few exciting developments on this front. There is an exciting new linac from United Imaging - not yet FDA approved - and the rest of this post will focus on them. In addition, there is an FDA approved linac by Linatech called Venus X, although I don’t see one operational in North America. I will have a post up in the next few days about them.
Let’s see what ChatGPT has to say about United Imaging:
United Imaging Healthcare (UIH), officially known as Shanghai United Imaging Healthcare Co., Ltd., is a prominent medical technology company headquartered in Shanghai, China. Established in 2011 by former Siemens employees Xue Min and Zhang Qiang, UIH specializes in developing and manufacturing advanced medical imaging and radiotherapy equipment.
The company's product portfolio encompasses a wide range of high-performance medical imaging products, including molecular imaging, magnetic resonance imaging (MRI), computed tomography (CT), digital radiography, angiography, mammography, mobile C-arm systems, and radiotherapy systems.
In 2013, UIH expanded its global footprint by establishing a research and development center in Houston, Texas, which later became its North American headquarters in 2018. The Houston facility, spanning nearly 100,000 square feet, includes a U.S. factory, product showroom, service training center, and service parts distribution center.
UIH has experienced significant milestones, including the installation of its 20,000th global system in New York in 2022 and the shipment of its 30,000th system globally from its Houston manufacturing facility in 2024. The company has also expanded its presence with an R&D office in Seattle and operations in over 75 countries, including Poland, the United Kingdom, Italy, Germany, New Zealand, Australia, India, Japan, and South Korea.
In August 2022, UIH held its initial public offering on the Shanghai Stock Exchange's STAR Market, raising approximately US$1.6 billion, marking one of the largest offerings in China that year.
UIH is committed to its mission of "Equal Healthcare for All" and continues to innovate in the medical technology field, collaborating with renowned institutions such as UC Davis and Washington University in St. Louis.
They have developed a product called uRT-linac 506c (it needs a better name - how about EvoBeam or Exacteon or Prismatica? Just spitballing). Let’s see what it can do:
The uRT-linac 506c is an advanced linear accelerator developed by United Imaging Healthcare (UIH), designed to integrate diagnostic-quality helical computed tomography (CT) with precise radiotherapy delivery. This integration facilitates a seamless workflow from simulation to treatment, enhancing the precision and efficiency of radiotherapy procedures.
Key Features:
Integrated Design: The system combines a 16-slice helical CT scanner with a C-arm linear accelerator, allowing for high-quality imaging and accurate treatment delivery within a single platform.
High-Quality Imaging: The diagnostic CT provides superior image quality with a large field of view and extended scan length, enabling detailed visualization of patient anatomy for precise treatment planning and delivery.
Advanced Radiotherapy Applications: The uRT-linac 506c supports various advanced radiotherapy techniques, including volumetric modulated arc therapy (uARC®), step-and-shoot intensity-modulated radiotherapy (sIMRT), dynamic IMRT (dIMRT), 4D-CT, non-coplanar treatments, and respiratory gating therapy.
Intelligent Radiotherapy Platform: The system features intelligent auto-contouring, automated treatment planning (Autoplan), and an intelligent quality assurance (QA) system, enhancing treatment planning efficiency and consistency.
Online Adaptive Radiotherapy: With the capability for online adaptive radiotherapy (ART), the uRT-linac 506c allows for timely adjustments to treatment plans based on anatomical and functional changes in the patient, ensuring optimal target coverage while sparing organs at risk.
Studies have demonstrated that the uRT-linac 506c exhibits good and stable performance in mechanical and dosimetric accuracy. The integrated CT system provides an efficient workflow for image guidance with submillimeter localization precision, making it a promising platform for advanced adaptive radiotherapy.
Please note that as of now, the uRT-linac 506c is not FDA or CE marked and is not commercially available in the U.S. or the EU.
Okay, so it can do basically everything our TrueBeam can do. But, instead of CBCT, it has integrated a diagnostic CT - i.e. fan beam CT - for image guidance. This machine can function as the simulator, using the IGRT images for planning (I have done a bootleg version of this with a TruBeam, but only for palliative cases as it is difficult to see OARs and targets well with a CBCT). It has automated planning software, its own QA system (I’d love a physicist to directly message me and explain this to me further, if they know what this means, exactly) and online adaptive RT.

(I had to figure out what fan beam meant vs cone beam; essentially, fan beam is the tech that a diagnostic CT uses and it acquires the data slice by slice, while a cone beam is looking at the data as a 3D volume. So, CBCT is typically much faster, has lower radiation dose but the image output is of lower quality than FBCT and can greater distortion from artifact)
There are a few publications about this machine out there. Here is one for our physicist friends, discussing its commissioning.
The study of interest to me was a case study about a nasopharynx cancer patient that they treated on this linac that required adaptive planning. They fused an MRI to the FBCT images obtained from the linac during simulation and contoured from that. Then, they performed the automated treatment planning using pre-determined constraints.
Given the challenges of planning design for NPC due to the tumor’s irregular shape and proximity to critical structures, previously treated high-quality plans were used as training data to develop a deep-learning model for predicting 3D dose distribution. The plan optimization algorithm utilized the predicted 3D dose distribution and a clinical goal sheet as inputs. To directly generate a deliverable and clinically acceptable plan without user intervention, the algorithm automatically integrated various optimization strategies and applied them as necessary. The algorithm includes a predictive adjustment feature that supports the manual adjustment of the AI-generated plan, providing greater flexibility and convenience. The medical physicist and radiation oncologist approved and evaluated the AI-generated plan. The initial and adaptive plans were assessed using the patient’s anatomy of the day (IGRT and ART plans) and compared using dose-volume histograms.
This is pretty cool! It appears they generated a fully acceptable treatment plan with no need for human intervention. They treated the patient with the generated plan up until fraction 24, when weight loss led to a significant mismatch between the target volumes and anatomy. So, using the FBCT and the automated treatment planning, they adapted the plan. You can see from the table below how the target coverage improves with the adapted plan:

You can also note that doses to most OARs were improved, as well:
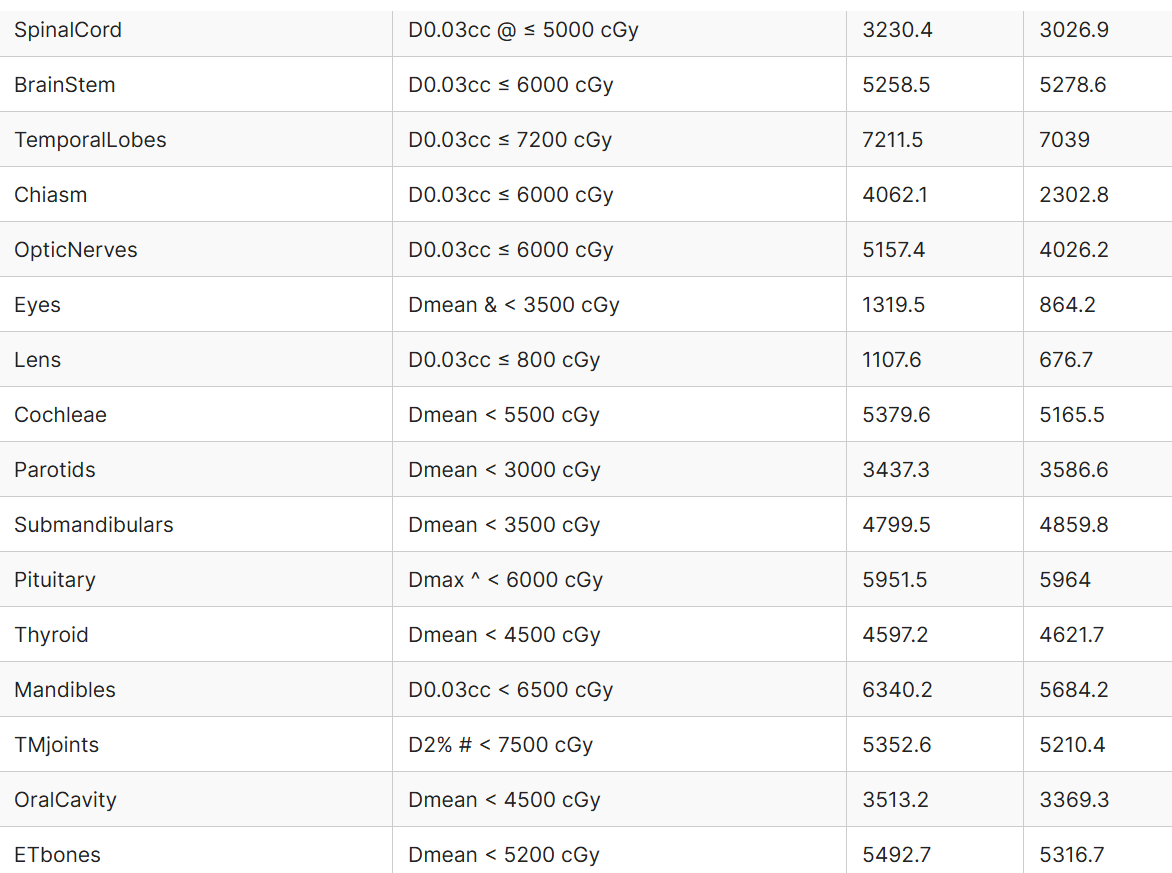
Here is how long it took the do the entire process:

Folks, this is <19 minutes from FBCT to treatment, including the recontouring and re-planning. What the actual f*ck!
For head and neck cancers, the proximity of the target volumes to numerous critical organs poses significant challenges in treatment planning. Online ART requires the rapid design of high-quality plans while the patient is positioned on the treatment table, making it a complex and demanding task. Yoon et al achieved a median online ART plan generation time of 19.5 min in a retrospective simulated environment [17], while Vladimir et al. reported a mean online ART time of 26.1 min in a clinical environment for head and neck cancer [15]. Both studies excluded the time for patient setup, image acquisition, and treatment delivery. In a randomized trial, the average time radiation therapists spent at the console (from radiation therapist arrival to quality assurance approval) was 22 min per online ART fraction [28]. For this patient, excluding CT scan and treatment delivery time, the total time for online ART was 11 min 54 s, confirming the feasibility of online ART using this novel integrated platform and the efficiency and accuracy of AI contouring and AI planning.
This machine can do adaptive planning and treatment in about half the time of what we currently have on the market.
I am impressed - I hope you are, too. This machine is years ahead of what we have on the market compared to existing products. If United Imaging is able to get this FDA approved, we may have some real competition for a premium workhorse linac. There are some issues I can foresee:
We are in the midst of starting a trade war with China. If the cost is similar or less to a Truebeam, tariffs may make it challenging to compete in the American market, which is the largest market for linacs.
Cybersecurity threats are real. TikTok is leaving the American market because of data security concerns. The same risks are present in health care and I foresee that this could be a challenge.
Varian has a near monopoly for the high end products and people are very familiar with their hardware / software. Even if it is the same or better at the same or lower costs, path dependence may make it a challenge to market this product.
The FDA is under new management with the new administration. Although there is talk of streamlining it, there is even more talk about firing government employees. The arduous task of getting approval will only be harder and this could delay entry.
There will always be quality concerns when a product, especially a health care device, comes from China. We know about past issues and there may be fear of potential quality issues, particularly when it comes to patient care.
Tech support will not have been built up and there will be no “institutional wisdom” that contractors can provide. Downtime could become an issue if they get even a sliver of market share and there is not enough support.
If they do get approval and actual sell a few units, unless they get enough to make it worth their while, they may not achieve enough market share to fully commit to the market. If this happens - quality, tech support and other issues will be a problem and perhaps a difficult one to mitigate.
Overall, I think competition is a good thing, however the challenges outlined above may make it challenging for United Imaging to gain a foothold in the market. That being said, if it truly is a better machine, technology will find a way.

Jeffrey Bundy is the CEO of United Imaging’s North American division. Mr. Bundy, if you read this, please do get in touch at simul.parikh@gmail.com. We would love to have you on “The Accelerators Podcast” to chat.
In a few days, I’ll spend some time discussing Venus X by Linatech.
Love you all,
Sim
Dr Parikh - Interesting enough to get me to open a SubStack account! See you around.