


2026 Radiation Oncology Coding and Reimbursement Changes
Breaking down what’s changing


ASTRO put out a blog post last week about code revisions and based on the verbiage, it was difficult to understand exactly what is going on.
Here is a ChatGPT summary:
Significant changes to radiation oncology reimbursement are anticipated for 2026, driven by updates to coding structures and practice expense valuations. The American Medical Association (AMA) has approved revisions to radiation treatment delivery and image guidance codes to reflect technological advancements in the field. Simultaneously, the Centers for Medicare & Medicaid Services (CMS) is updating the practice expense component of the Medicare Physician Fee Schedule (MPFS), which has remained unchanged since 2010. These updates aim to ensure that reimbursement rates accurately reflect the current costs of providing radiation therapy services.
Key Changes:
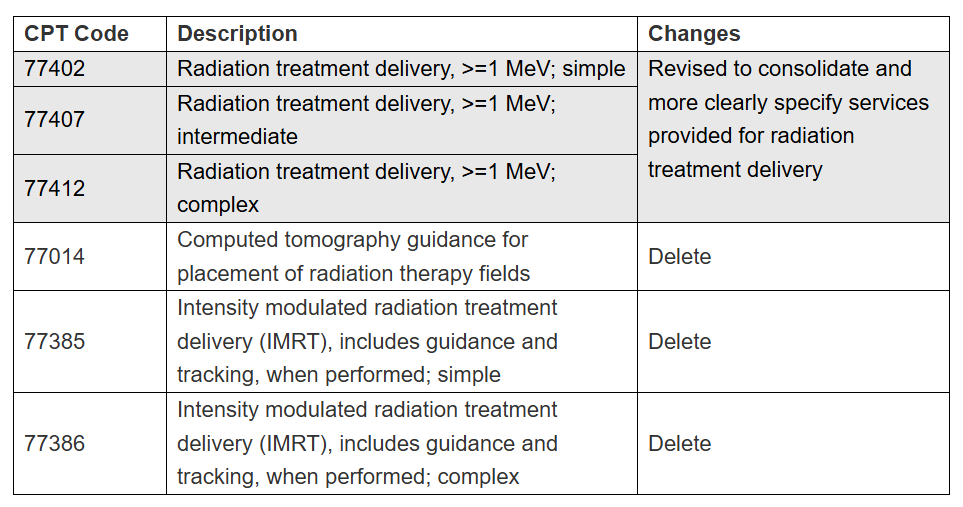
Coding Revisions: The AMA's CPT Editorial Panel has approved significant changes to radiation oncology treatment delivery and image guidance codes. For example, codes like 77402, 77407, and 77412 have been revised to consolidate and specify services provided for radiation treatment delivery. Additionally, certain codes such as 77014 (Computed tomography guidance for placement of radiation therapy fields) and 77385/77386 (Intensity modulated radiation treatment delivery) are slated for deletion.
Practice Expense (PE) Updates: CMS is updating the PE component of the MPFS, which accounts for a significant portion of radiation oncology reimbursement. The AMA's Physician Practice Information Survey (PPIS) suggested bundling radiation oncology practice expenses with those of diagnostic radiology and other specialties, potentially leading to a 40% reduction in the PE/hour rate for radiation oncology. This could undervalue the substantial capital expenses associated with radiation therapy.
Here is a chart from the post:
So, I did a little digging to understand exactly what all this means. Please forgive any errors, as I was not in the room. Feel free to send corrections and I will make the changes.
Audits have taken place over the years, and the use of certain codes has dramatically increased—particularly for simple/complex IMRT treatment delivery and IGRT. So, the powers that be decided to make some changes. The code deletions don’t mean we won’t be reimbursed—they will simply have different codes, some of which will be bundled.
The Changes
Isodose complex and electron treatments will be considered as simple treatment delivery. These don’t require any imaging or respiratory management. This code will rarely be used.
3D/IMRT with a single isocenter will be considered intermediate delivery. 77014 will not have to be added - it will be bundled. These cases will not include respiratory management or surface guidance. Basically, this will become our “bread and butter” code for much of palliation and curative radiation.
3D/IMRT with multiple isocenters or DIBH or surface guidance will be considered complex treatment delivery. IGRT, as with intermediate treatment delivery, will be bundled. This will be a significant proportion of our billed codes, as well.
All of these codes will get a dollar amount and a potential RVU re-valuation. This will be for both the technical and the professional reimbursement (i.e. 77014 will no longer exist for either and will be bundled into the other codes).
The practice expense reduction occurred because we did not submit enough responses to the PPIS surveys. Because the number of responses was so low, we were forced to join with radiology. The problem is that they use their diagnostic machines much more of the day than we do - i.e. the utilization is much higher, because radiology may be using their machines all day and even at night, while we only use ours from 7a-8a to 4p-5p. So, our practice expense value will be lower than the reality of the value. My understanding is that reimbursement is calculated as X per hour and so we will receive X × 8 hours, while diagnostic radiology will receive X × 24 hours.
There are some other changes to our practice expenses that will be in our favor - but this will be less than the above. Our linac costs have increased (Truebeams cost a lot more than an iX, for example), we have to buy expensive equipment to treat our patients (motion management, prone breast boards, surface guidance and more), and labor costs have all risen. Hopefully, these costs will be valued at a higher rate.
Now, what does all this mean? Well, we simply don’t know. I sincerely believe ASTRO is correct in that we may all be getting a tremendous haircut. This has happened in the 2015 revisions. Here is the ChatGPT summary:
Key Changes in the 2015 Radiation Oncology Code Restructuring:
Elimination of "Stacked" Codes:
Prior to 2015, radiation oncology procedures were billed using multiple separate CPT codes for different components (e.g., treatment planning, physics, and dosimetry).
The 2015 overhaul bundled several of these services into new comprehensive treatment codes, reducing the number of billable codes and impacting reimbursement.
New and Revised CPT Codes:
Several old codes were deleted and replaced with new, consolidated codes for:
3D Conformal Radiation Therapy (3D-CRT)
Intensity-Modulated Radiation Therapy (IMRT)
Image-Guided Radiation Therapy (IGRT)
Stereotactic Radiosurgery (SRS)
Brachytherapy
The goal was to streamline coding and reimbursement but ultimately led to reduced payments for some procedures.
Significant Reimbursement Reductions:
The changes resulted in major cuts to payments, particularly for IMRT and SRS/SBRT, as CMS adjusted work RVUs downward.
Many private practices and freestanding radiation therapy centers faced financial strain due to the lower reimbursement.
Introduction of Physics and Dosimetry Bundling:
Previously, medical physics and dosimetry services were often billed separately.
The new structure bundled many of these services into broader codes, reducing the number of separately billable physics-related codes.
Growing Shift Toward Alternative Payment Models:
The 2015 adjustments laid the groundwork for value-based care models, including discussions that led to the eventual Radiation Oncology Alternative Payment Model (RO-APM), which CMS proposed in later years.
Impact of the 2015 Code Changes
Hospitals and larger academic centers were somewhat insulated, but freestanding radiation oncology clinics suffered the most.
The cuts led to practice closures and consolidation of radiation oncology services into larger healthcare systems.
It set a precedent for future reductions in radiation therapy reimbursement, leading to the 2021 updates and the ongoing discussions for 2024+.
After 2015 is when the treadmill started getting faster and faster, yet many of us earned less money for seeing more patients than before. Even before this, we were seeing signs of consolidation, but the pace of it picked up quickly afterwards. Because freestanding was hit harder, hospitals bought the centers / certificates of need and began to bill under hospital codes. PPS-exempt centers expanded and billed at their higher rates, as there was a “grey area” of how affiliates/network sites could bill and they were able to maintain their high reimbursements, while many other centers struggled, sold to hospitals or closed down. Freestanding centers that survived ran lean and became a volume business. There are rarely hospital centers that treat 30+ patients, but freestanding centers routinely treat that many or more. People note that freestanding centers tend to use more fractions, but they still tend to be higher value than hospital outpatient centers. Oftentimes, 10-15 fractions for a bone metastasis at a freestanding center are reimbursed at a lower rate than 1-5 fractions at a hospital-based department.
What Could Happen
The net changes in the value of the codes stays about the same or increases and not much changes for practices. ROCR becomes unnecessary and the will to push for legislative changes will diminish.
OR
The net changes in the value of the codes decreases substantially and this destabilizes practices, with freestanding again taking the brunt of the pain. ROCR becomes absolutely crucial.
Until July 2025, we won’t know which of these will be the case. However, the case rates that have been developed for each of the nine cancers in ROCR are based on today’s reimbursement. If ROCR does not receive a CBO score now, obtaining one after the code restructuring may be problematic. If each cancer is reimbursed at a lower rate based on the newest code valuations, then the CBO score will show that ROCR is far more expensive than the status quo, rather than the $200 million in projected savings over 10 years that they now estimate.
Am I a gambler? Not really. I’d rather take less now than try to get more later with the risk of a tremendous haircut. Yet, as I’ve repeatedly said, the same people trying to fix this mess are the ones who created it. If we didn’t exempt protons and were able to rescind the PPS exemption, we would save far more money and the CBO scoring would be moot. So, at this time I prefer we get ROCR scored by Congress expeditiously. With all the fires going on the world, I suspect that this is not going to be high priority.
Some Food For Thought
Finally, accreditation remains an integral component of ROCR. I have been digging to understand this. Yes, the government is becoming more interested in “quality” (heavy finger quotes). However, no specialty’s entire payment is rewarded or penalized based on this. Industry is concerned about payment reforms. If reimbursement is bundled, the business incentive to modernize or upgrade technology is reduced. If clinics decide not to upgrade their technology or buy new linacs, then industry will also feel pain. I have a feeling that industry is pushing for accreditation to be mandatory and that they will also require certain technology and newer equipment to be a part of meeting practice parameters. If this sounds too conspiratorial to you, you may be right. It’s just that I have heard this from multiple sources and it makes some sense to me. As I’ve said, accreditation does not appear to have any effect on patient outcomes, the most important criterion in the Donabedian model; the other two are structure and process.If you have interest in quality in medicine, I strongly recommend reading this seminal paper.
Some Culture Recommendations
Read: The Three Lives of Cate Kay, a great novel about Hollywood, novelists and young love.
Listen: The Lumineers have a new album finally! Automatic. I think “A—hole” is my favorite right now.
Watch: Landman, a riveting show about oil and gas in West Texas. Has a real Friday Night Lights feel. Texas Forever!
A Personal Note
I’m moving on to a job closer to my home. That’s number five for me - I plan on writing about my moves at some point in the future. I know that seems like a lot for a guy 15 years out, but I’ve always felt that jobs were like clothes - when they stop fitting, it’s time to find something new and more comfortable. Lake Huron Medical Center was a lifeline for me and I will continue to provide support and coverage, but I am excited about my new adventure. Wish me luck! I get to work with the doctor that wrote my first LOR for residency and a few legends in our field. Oh, our pup Bella is doing great. Not quite potty trained yet, but almost there and she has become Silas’ right hand gal.
Love you all,
Sim
(If you get this forwarded to you by friends or come across this another way, please do subscribe. It costs you nothing, but occasionally I may write something of interest to you)
If you read the publications by the AMA, this was decided in the fall and we are just now somehow hearing about it:
https://www.ama-assn.org/system/files/sept-2024-summary-of-panel-actions.pdf
Codes 77014, 77385, and 77386 are being deleted.
Codes 77402, 77407, and 77412 are being modified.
Currently, the only one of those codes that has a professional component is 77014 when you bill it with -26 modifier. This code represents 25% of my revenue. Deleting this code without assigning at least 0.85 wRVU to the 77402/07/12 codes would be catastrophic to me and anyone else who is compensated on a productivity model in any way.
At this point, we are only guessing that a professional component will be able to be billed for codes 77402, 77407, and 77412. This should have at minimum 0.85 wRVU of value. Will it? Fool me once, shame on you...
I think that's pretty clear that's why this is going on. Who made this decision, and who exactly is the AMA looking out for?
And ASTRO? ROCR? Seriously? Again? Why do those who consider themselves our betters think they can carve out our specialty from CMS payments to be different than literally every other specialty? And forcing accreditation? This comes back to their hard on for babysitting linacs and killing general supervision to prevent doctors from having responsibilities at multiple sites -- something completely tone deaf to the needs of rural practice, and more than anything it creates a literal racket that drives up costs. it's antithetical to free markets and hopefully something the anti-bureaucracy present regime will shoot down but I won't get my hopes up.
What ASTRO NEEDS to be focusing all of its efforts on right now is assuring 77402, 407, and 412 all have at least 0.85 wRVU assigned. Instead they are screeching about ROCR and totally missing the forest for the trees. ROCR is not the solution. The wRVU component for those codes is. To at least maintain status quo in a time of crisis.
Who's looking out for you? It's not ASTRO or the AMA, that's for sure.
So, if the 3D and IMRT treatment delivery codes are going to be combined, what happens to the planning codes? Code 77301/77338 will now be reported with treatment delivery codes 77407-77412? Any change to any of the G codes since they can also be reported for IGRT, not just 77014?